Mid-Atlantic Support Group Social Brings Families Together
 On August 11th, the Mid-Atlantic Support Group held a summer social get together in Chadds Ford, PA. The gathering consisted of 22 families, 21 individuals with a variation, and over 50 attendees total. Families came from Massachusetts, New York, New Jersey, Pennsylvania, Maryland, Delaware and California. Children and adults representing XXY, XYY, XXYY and Trisomy X enjoyed a cook-out and various indoor and outdoor games. For some, it was the first time ever meeting someone else with their condition. For others, it was an opportunity to catch up with friends.
On August 11th, the Mid-Atlantic Support Group held a summer social get together in Chadds Ford, PA. The gathering consisted of 22 families, 21 individuals with a variation, and over 50 attendees total. Families came from Massachusetts, New York, New Jersey, Pennsylvania, Maryland, Delaware and California. Children and adults representing XXY, XYY, XXYY and Trisomy X enjoyed a cook-out and various indoor and outdoor games. For some, it was the first time ever meeting someone else with their condition. For others, it was an opportunity to catch up with friends.
Ryan Bregante, who started the group Living with XXY, attended after having spent the week participating in a study at the NIH. He shared his positive experience with everyone interested, encouraging them to participate in research studies if they could. A number of the young adults were excited to have the opportunity to talk with Ryan face-to-face. It was also educational for Ryan to meet those with other conditions.
Mostly, it was an opportunity for people to talk and interact in a social environment with others just like them. Both parents and individuals with one of the conditions, found the afternoon to be an opportunity to learn new things, make new friends, and leave the rigors of daily life behind for a few hours.
This comment from one parent perhaps captures the essence of the day best of all. “I got very emotional watching Violet speak, for the first time ever in person, with another girl with Trisomy X. I remember being so scared when we first found out her diagnosis, not knowing anything about it and feeling so alone. Having the opportunity to watch her play with another girl with her condition was incredibly moving. They seemed to have an immediate connection with each other. Violet said on the way home that they “just started talking and were friends right away.”
Sometimes navigating through the ‘regular world’ can be challenging when people don’t understand why Violet acts the way she does. Being with a group of people who understand is very comforting. These kinds of meetings are so valuable both for opportunities like Violet’s, and also for the relationships built between parents with shared experiences.”
Another parent had this to say, “It was life changing for us as a family, and it will be an incredible support system for Carlos as he grows up. We are so grateful for all of you and what you do; for providing this platform to interact and support one another. Thank you so much for having us. Carlos is still talking about it.”
 And this from a teen, “I went to a meet and greet, where I could meet other men that can relate with me. I met a guy named Ryan who has a YouTube channel and explains what living with XXY is like. Even though I have XYY and most of the men at the meet and greet have XXY we all have experienced similar events in our lifetime. This has changed the way that I see myself, knowing that someone else understands how I feel. It was a moving experience for me.”
And this from a teen, “I went to a meet and greet, where I could meet other men that can relate with me. I met a guy named Ryan who has a YouTube channel and explains what living with XXY is like. Even though I have XYY and most of the men at the meet and greet have XXY we all have experienced similar events in our lifetime. This has changed the way that I see myself, knowing that someone else understands how I feel. It was a moving experience for me.”
And from his mom, “Me as a parent for the first time got to meet other parents with X and Y chromosome variations. It makes me feel like I’m not alone and we have so many similar stories, struggles, triumphs and love for our children. We can only move forward to help our children as a larger voice and making a person living with these variations feel valued and not ashamed for being different. This meeting was amazing to see how far awareness has come but we have so much more to do. Thanks for making the gathering possible. I will be at many more….”
As an added bonus, those attending contributed $300 towards food costs, which has been donated to AXYS on behalf of the group.
Everything You Never Knew About the ADHD Brain
Article Title: Everything You Never Knew About the ADHD Brain
Author: Alison Kravit, PsyD, AAC
Date of Publication: July 2018
“Imagine hundreds of cars approaching an intersection that has no traffic light or stop sign. This is what happens to the ADHD brain every day where the prefrontal cortex (the intersection) is unable to properly regulate your various thoughts and feelings (the various cars approaching the intersection). Learn more about the ‘Intersection Model’ for ADHD.”
Secrets of the ADHD Brain: Why We Think, Act, and Feel the Way We Do
Article Title: Secrets of the ADHD Brain: Why We Think, Act, and Feel the Way We Do
Author: William Dodson, MD
Date of Publication: 2016
“ADHD is a confusing, contradictory, inconsistent, and frustrating condition. It is overwhelming to people who live with it every day…The Diagnostic and Statistical Manual of Mental Disorders has 18 criteria, and other symptom lists cite as many as 100 traits.”
The Brain-Behavior Connection In Children with ADHD
Article Title: The Brain-Behavior Connection In Children with ADHD
Author: Joel Nigg, PhD
Date of Publication: 2016
Presentation slides providing information on the neuroscience of attention and emotion as it relates to ADHD. The slides also offer a look at self-regulation of emotions and behavior in individuals with ADHD and how much variability there is in this condition from one child to the next.
Early Intervention for Infants and Toddlers with X & Y Variations
The Early Intervention Process
The Early Intervention Program for Infants and Toddlers with Disabilities is the program known as Part C of the Individuals with Disabilities Education Act (IDEA). It is also known as Child Find.
Part C is a federal grant program that encourages states to set up programs for young children with disabilities and their families. Currently, every state has a Part C program.
To find a program near you, talk to your child’s doctor or call your local public school.
For more information, please see these Federal Technical Assistance for Early Learning resources from the U.S. Department of Education.
Referral to Part C
Parents can request a free evaluation if they are concerned about their child’s development. Other people can also make this request on behalf of parents, but no evaluation or services can take place without parental consent. This aspect is optional for states.
Screening of the Child
This is a quick look at how your child is developing. Your child’s doctor can do this. This is an optional activity for states.
Assignment of a Service Coordinator
The service coordinator is responsible for implementing the IFSP and will work with the family while they receive Part C services.
The Multidisciplinary Evaluation and Assessment
The evaluation and the assessment are often done at the same time.
The Multidisciplinary Evaluation
- In order to determine the child’s eligibility for services, a multidisciplinary evaluation takes place by a team that may include speech-language pathologists, audiologists, occupational therapists, physical therapists, psychologists, social workers, and early intervention specialists.
- A variety of procedures are used to determine if the child is eligible for services. They include observations, tests, interviews, play-based assessments, checklists, and other items.
- A diagnosis of an X and Y variation may enable the child to receive services without an evaluation.
The Multidisciplinary Assessment
- Once eligibility is determined, a multidisciplinary assessment is completed that may include the same people who did the evaluation.
- An audiologist may perform a hearing test, as ear infections are common in this population.
- Occupational therapists may observe fine motor areas such as the grasp, states of alertness and overload, reactions to sound, light, and touch, and other sensory-motor areas.
- Physical therapists may watch for balance, gait, posture and movement issues.
- Speech pathologists attempt to determine both receptive (listening) and expressive (speaking) language levels. If the child is not yet talking, the speech pathologist may try to determine language comprehension using augmentative language devices (picture boards, etc.).
Parent Preparation
- Parents are an integral part of the team, and their input is vital. Parents need to make the team aware of conditions that will help lessen anxiety— such as making the environment calm and free of distractions and sensory overload.
- The assessment may take place in the child’s home, where the team member brings toys and test materials for administration in a familiar environment. It can also take place in a school or special education center, with the parents and professional team members participating.
- Parents can prepare for the process by learning as much as they can about unfamiliar concepts and terminology, talking to other parents about the process, and writing down their questions and concerns.
- It is important for parents to realize that they know the most about their own child and may know more about X and Y variations than some of the professionals on the team. Parents may wish to bring brochures about X and Y variations, the website address of AXYS, and other materials to share with and educate team members.
Questions to consider prior to the assessment
- What time of day is your child at his or her best?
- Will your child be overwhelmed by strangers in strange places? Might it be preferable to conduct the assessment in your home?
- Who will be conducting the procedures, and what are their roles?
- What types of tests will they use, and what do they measure?
- Are formal tests the best way to determine your child’s strengths and weaknesses? Would more informal, play-based assessments be more effective?
- How long will the assessment take?
- What helps calm your child to ensure his or her participation?
- What should you bring with you? Favorite foods, toys, videos of your child in various situations?
The Individualized Family Service Plan (IFSP)
This is a written plan that details the early intervention services.
- The IFSP must be created within 45 days of the referral, be reviewed every six months or more often if needed, and formally evaluated on an annual basis.
- No services are provided without the written consent of the parents.
Preparing the IFSP
- After the assessment, a meeting is held with the parents and all the professionals involved. The team will present test results, including scores, observations, and recommendations for services.
- Parents may be surrounded by a variety of special educators and may be intimidated and hesitant to contribute to the discussion. However, given that parents know their own child better than anyone and may extensive knowledge of X and Y variations, should approach the meeting as partners in decision-making, not as recipients of the special education team’s decisions.
- Parents should also bring their lists of concerns for their child and ideas for goals.
- The team, including the parents, will write a plan for addressing the unique needs of the child and family. This document is the Individualized Family Service Plan.
IFSP Content
- Description of the child’s current development.
- The family’s resources, priorities, and concerns.
- Outcomes expected, and how the family might make progress toward reaching them.
- Services needed to help the child and family reach the outcomes discussed, including length, duration, frequency, intensity, and method of delivering the recommended services.
- Statement that the service is provided in the natural environment to the extent possible.
Possible Early Intervention Services
- Assistive Technology
- Audiology
- Family Training, Counseling, and Home Visits
- Health Services
- Medical/Nursing Services
- Nutrition Services
- Occupational Therapy (OT)
- Physical Therapy (PT)
- Psychological Services
- Respite Care
- Service Coordination
- Social Work
- Special Instruction
- Speech-Language Pathology (SLP) Services
- Transportation
- Vision Services
Types of Goals for Infants and Toddlers
- Physical therapy goals might include those that help with low muscle tone, including posture and feeding.
- Speech-language pathologists will help with receptive and expressive language goals, working on comprehension of language and means of expression, whether verbally or with augmentative devices (such as pictures, language boards, or signs).
- Occupational therapists help with a variety of sensory issues such as over- sensitivity to touch, noise, crowded rooms, and certain lights. They can also help with sleep issues.
- Occupational therapists and speech-language pathologists may contribute ideas for oral-motor stimulation to help sucking, chewing, and swallowing.
- Early intervention specialists can help design goals to stimulate early play and cognitive development.
- Social workers and psychologists should be available to help the family cope with the diagnosis and intervention needs.
Where Services Are Provided
- The services should be provided in the child’s natural environment, including the home and community environments that are typical for infants and toddlers of the same age who do not have a disability.
- The family can provide information where their everyday activities occur. For example, natural environments can include the home, neighborhood, parks and recreation centers.
- When services are offered in the home, various professionals can teach activities to parents and/or caregivers and have them practice with the child between sessions (speech games, feeding ideas, massage, exercises, etc.).
- For services not provided in natural environments, the IFSP must state why.
How Services May Be Provided
- Speech pathologists need to work with occupational therapists to ensure that the child’s sensory needs are considered when addressing feeding and talking.
- Speech therapists and early intervention specialists may work together to create augmentative communication devices (picture boards, etc.) for children who are delayed in learning to talk.
- For children with X and Y variations, it is important to establish a routine with all provided services. This helps greatly in reducing their anxiety.
- The various therapists and teachers should also provide visual cues to help children anticipate and follow the sequence of their visits. If the speech/language pathologist comes to the home every week, it can be helpful if she or he always brings a bag of toys or a certain stuffed animal. This helps your child identify and anticipate the visit. When the therapist maintains a specific visual schedule, the child learns to adapt and participate more readily.
Family Rights
- Parents should be provided with written copies of their rights under Part C.
- Parents should receive copies of all written reports and records.
- Parents must give written consent for the child’s evaluation and prior to the child receiving services.
- If parents have a concern or complaint, they should talk to their service coordinator and the service provider.
- If resolution cannot be reached at the informal level of discussion, then the parents or professional involved have formal remedies of mediation, including the filing of complaints and an administrative hearing, if needed.
Additional Information
Download the model IFSP form published by the U.S. Department of Education.
Transition Plan at Age 3
Requirements
- A transition plan must be developed for the child as part of the IFSP no later than 90 days prior to the child’s third birthday to ensure the smooth transition into Part B services.
- At age 3 the services a child with a disability receives are provided by the preschool programs through the local school district—also known as Part B of IDEA. There is also an eligibility process at this stage if parents want their child to start or continue receiving services.
Ideas for Parents
- At the time of this transition, families need to explore and visit available options for their child’s educational services. School systems may offer a variety of services for preschoolers with special needs. They may offer some special education within a regular preschool class. They may also have early childhood special education classes, where all of the children have some type of developmental delay or disability.
- For the child with FXS, parents need to look at the setting, services, and personnel involved in the early childhood program. Multidisciplinary services offered in a structured, calm setting, with an established routine, many visual cues, and provision for calming places and activities are all important for the preschooler with FXS.
Website Resources
- Federal Register – Part C of IDEA
- National Dissemination Center for Children with Disabilities – Babies & Toddlers
- Wrightslaw – Early Intervention (Part C of IDEA)
Thank you to the National Fragile X Foundation for allowing AXYS to use this content.
OT, SLP, AT & The IEP… Making Sense of the Alphabet Soup
Creating an IEP – or Individualized Educational Program – can be an incredibly confusing and daunting experience. The “alphabet soup” of acronyms and legalese often increases the anxiety and uneasiness for families. There are often many professionals in the room, some just popping in and out during the meeting, and families can feel isolated and not fully part of the process. One way to offset these feelings is to prepare ahead of time.
We’ve designed this article to be an at-a-glance format, combining our professional expertise and some handy resources. This information is presented via FAQs (more alphabet soup for frequently asked questions) and IEP insider tips. In addition, we have included voices and insights of families from the NFXF community and their perspectives based on personal, first-hand experiences about the IEP process. We’ve kept the families anonymous and sincerely thank them for their valuable comments and suggestions. All family contributions are italicized so you can quickly find them.
Be sure to check out the many handy resources at the end. It is our sincere hope that families can find some helpful information to aid them in confidently participating in your child’s IEP as a key member of the team.
Frequently Asked Questions
What is IDEA – Individuals with Disabilities Education Act? And Now IDEIA – Individuals with Disabilities Education Improvement Act?
IDEA / IDEIA is the federal law that makes special education available for students with special needs.
What are FAPE (Free and Appropriate Public Education) and LRE (Least Restrictive Environment)?
FAPE – Free and Appropriate Public Education: FAPE is central to the federal law and is a protected right of children eligible for special education. Just like all other children, students with special needs have the right to a free public education.
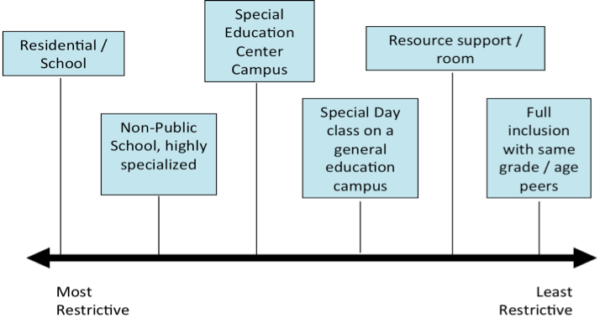
LRE – Least Restrictive Environment: This means that schools must consider teaching a child with special needs in general education whenever possible. There is a continuum of “restrictiveness” ranging from the most restrictive of residential placements, to special education centers where all children on the campus have special needs, to special education classrooms on general education campuses, to resource style classes where students spend parts of a day in special education and parts of the day in general education and full inclusion in general education settings. The graphic is a representation of “restrictiveness”.
What is an IEP – Individualized Educational Plan or Program?
An IEP is a written statement for each child with a disability, and it is developed, reviewed and revised according to the requirements of IDEA.
IEPs are typically held once per year, but the timing may vary depending on the needs of your child.
Tip: You can call an IEP meeting any time.
IEPs typically have a flow of how things will proceed. Each team is different, but generally the team should use the following flow for discussing the student’s educational program.
- IEP team must collaboratively brainstorm to identify needs within the PRESENT LEVELS OF PERFORMANCE.
- areas of identified need, the team must develop GOALS AND OBJECTIVES.
- Once completed, THERAPY SUPPORTS are discussed and documented that may be necessary in order to meet the agreed upon goals and objectives.
What is Speech Language Pathology (SLP)? Is that the same as Speech Therapy (ST)? What is a Language, Speech and Hearing Specialist (LSH)? What do I need to know about Speech and Language?
Often in schools, SLP, LSH and ST are used interchangeably – BUT the training and degree are the same. Typically LSH is only used in school settings.
Communication is an UMBRELLA that includes many concepts. Here is a breakdown that we find helpful.
What is Speech?
Speech includes: production of phonemes (sounds), voice and fluency. In other words, articulation.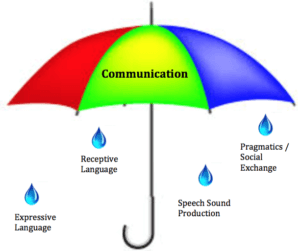
What is Language?
Language is the area of functioning that is most crucial for all aspects of cognitive and social development. Language is comprised of Receptive Language and Expressive Language.
- Receptive Language: The understanding – or what the individual receives via communication in the environment. Receptive Language includes both verbal and visual input.
- Expressive Language: Ability to communicate – express – wants and needs. Expressive Language includes both verbal and visual input.
What are Pragmatics?
Pragmatics: The use of language or may be referred to as, “social language” (e.g. taking turns, waiting, sharing, eye contact, facial expressions). Pragmatics also includes flexibility of thought and language use depending upon the situation.
What are Speech Therapy services in schools most concerned with?
- Socialization /Pragmatics
- Design of a Language Rich Environment
- Emphasis is to encourage language through various modalities on an everyday basis.
LSH therapists are support staff who can assist in the development of communication tools, which should be used on a consistent basis and embedded into the IEP.
What is Occupational Therapy?
- The term “occupation” comes from how we “occupy” our time. Our daily life’s roles and activities including self-care, play, work, social engagement, leisure, and learning are all daily “occupations”.
- OT services are provided to a student if those supports are needed to meet annual goals as outlined in the IEP. In school settings, OT’s support student learning, access to and overall participation in educational settings and routines including academic and non-academic domains.
- Sensory Processing differences often greatly impact one’s fulfillment of daily occupations.
What is Sensory Integration (SI)?
- Sensory Integration (SI) is defined as:
The organization of sensation for use.{{1}} - SI issues also known as sensory processing differences impact:
- Attention and focus
- Behavior
- Language processing
- Learning
- Overall functioning
- Research has well documented SI issues in many individuals with FXS.
What is Assisted Technology (AT)?
- According to IDEA 2004, AT is defined as:
Any item, piece of equipment, or product system, whether acquired commercially off the shelf, modified, or customized that is used to increase, maintain, or improve functional capabilities of children with disabilities. - AT must be considered on EVERY IEP.
What is Augmentative and Alternative Communication (AAC)?
- AAC is part of AT that focuses on communication.
- AAC is not just a “device that talks” but includes a broad spectrum of applications including symbols, gestures, pictures, icons to enhance communication.
- Use of AAC applications will NOT stop someone from talking.
BEFORE the IEP Meeting
What to ask for in advance:
- Ask for an IEP agenda.
- Ask for draft copy of the IEP in advance including present levels and proposed goals.
- Ask for assessment reports in advance.
*NOTE* Requests for present levels, goals and assessments prior to the meeting may need to be in writing. This can often be done via email and/or by dropping off a note at the school. Be sure to find out how much advance notice is required in order to have your requests honored and to allow the school team to adequately prepare your drafts. This can vary by district (e.g. 3 days, 1 week).
Prepare your own thoughts about your child’s present levels. Have strengths and areas of concern in mind. Consider bringing this information in a handy note format that is comfortable for you to share with the team. (See Positive Student Profile – below)
DURING the IEP Meeting
Go in as a collaborator not as an adversary.
YOU are the best source of information on your child and his/her best advocate
- Begin with your child as an individual who has strengths and gifts
Ask to have the IEP notes read aloud at the end of meeting with ALL team members present. This helps to make sure the team is all in agreement about what was discussed and will help to clarify any issues.
Pointedly discuss collaboration DURING the IEP meeting. Put it ON the IEP as part of the service delivery. For example:
- Schedule team meetings monthly or quarterly.
- Define expectations for team communication (e.g. logs in notebooks or email).
- Many therapists & teachers have good intentions, but unless we have formal COLLABORATION SPACES, TIME and PLACES, it may not actually happen in the way we all want it to happen.
You do NOT need to sign the IEP right away at the end of the meeting
- You can take it home, review it, share with partner/family and sign later
Many families make this their regular practice, not just when things are contentious}.
Positive Student Profile Examples
Tips from Parents on Meetings
- My input as a parent is really important in the IEP. So, I always write a detailed page for the “Parent Concerns” section. All year long I add bullet points to a document I keep on my computer. When something comes to mind – a particular challenge, a great success, a dream for him – I type a bullet point. Then when it’s time to write my part of the IEP, I have my bullets to refer to. I try to do my piece well in advance of the meeting in hopes that his teacher might use some of my thoughts to form the goals.
- I always tried to act as another part of the whole team. I did things, I volunteered to provide things, and expected others to do the same. I never went in just pounding my fist and requesting unrealistic things. It has to be cohesive!
- It never hurts to ask for something, the worst they can say is “No”.
- Trust your gut.
- Educate the IEP team on FXS and what you as the parent know about FXS learning styles each year.
Goals
Questions to ask about goals
- Ask what the goal will “look like” during the school day.
- Provides context.
- Ask about how skills will be generalized.
- Ask about how/when progress will be updated and what the parent – school communication piece will be.
- Ask about how the goal will be measured AND how that data will be collected and shared.
Goals should be
- Interdisciplinary
- Not just a “speech goal” or “OT goal”.
- Functional, measurable and data driven.
- The measured behavior should be clear so anyone reading the goal knows what it is.
- HIGHLY individualized to your child.
- For more information, please read Preparing for Your Child’s Individual Education Program (IEP).
Tips from Parents: Food and IEPs are a great pairing!
- For every meeting (monthly or IEP) we bring food. Muffins, scones, cut up fruit-yogurt and paper bowls since we usually meet in the early morning. We know their dietary needs as well and provide something healthy. It lets them know that we care about them and appreciate their help.
- I believe it’s a nice gesture AND it’s harder to say no with a bagel in your mouth. Pete suggests bringing enough so there is extra. Then when it’s in the teachers’ lounge and someone says, “Where’s this from?” The answer shows your generous parents as opposed to the talk in the teachers’ lounge being about your list of demands. We bring food in as well. I always come in a few minutes early and stop in the front office and make sure the secretary and principal have some as well as anyone else on the team who may not be at the meeting (like the paraprofessionals!). These small gestures have always helped not just with IEP’s but also throughout the year because they all KNOW me so when we have had to be firm about a decision they understand a little better. They are also more likely to go out of their way for us. 😊
AFTER the IEP
- COLLABORATE and follow through!
- Actively engage in the agreed upon team communication strategies – you are a key team member!
- Don’t hesitate to ask follow up questions. Remember, you can call an IEP meeting at any time, so if you want to meet again with the team, that is your prerogative.
Resources
IEP Information – www.understood.org (previously known as the National Center for Learning Disabilities, NCLD)
Chapter 7: IEPs – Developing Your Child’s Education Plan
Center for Parent Information and Resources (includes Spanish translation)
Raising Special Kids
American Speech & Hearing Association (ASHA)
American Occupational Therapy Association (AOTA)
Assistive Technology
Authors
 Laura Greiss Hess, PhD, OTR/L
Laura Greiss Hess, PhD, OTR/L
is an assistant professor in the department of occupational therapy at Dominican University of California. She began her career as a special education teacher in 1992 and then became a school-based occupational therapist in 1998. She worked at the UC Davis MIND Institute for 12 years on the FXS team under the mentorship of Randi Hagerman. Laura’s research and practice interests include: neurodevelopmental disorders such as Fragile X syndrome and autism, examining intervention outcomes as measured in daily life contexts with schools and families, interdisciplinary team collaboration, sensory processing and assistive technology applications.
Kerrie Lemons Chitwood, PhD, CCC-SLP
is a licensed speech language pathologist with 18 years of clinical and research experience. Kerrie currently is an adjunct professor in the Education Department at California State University, Monterey Bay (CSUMB). In addition, she is the program coordinator for the Masters of Arts in Education at CSUMB. Previously, from 2002-2012, Kerrie worked at the UC Davis MIND Institute, where she was part of the Fragile X team. She values intervention research and has extensive experience working as an integral member of a collaborative interdisciplinary team. She is committed to translational research and thrives to bridge the gap between research and practice specifically as it pertains to students and families with FXS and other neurodevelopmental disorders in various educational settings.
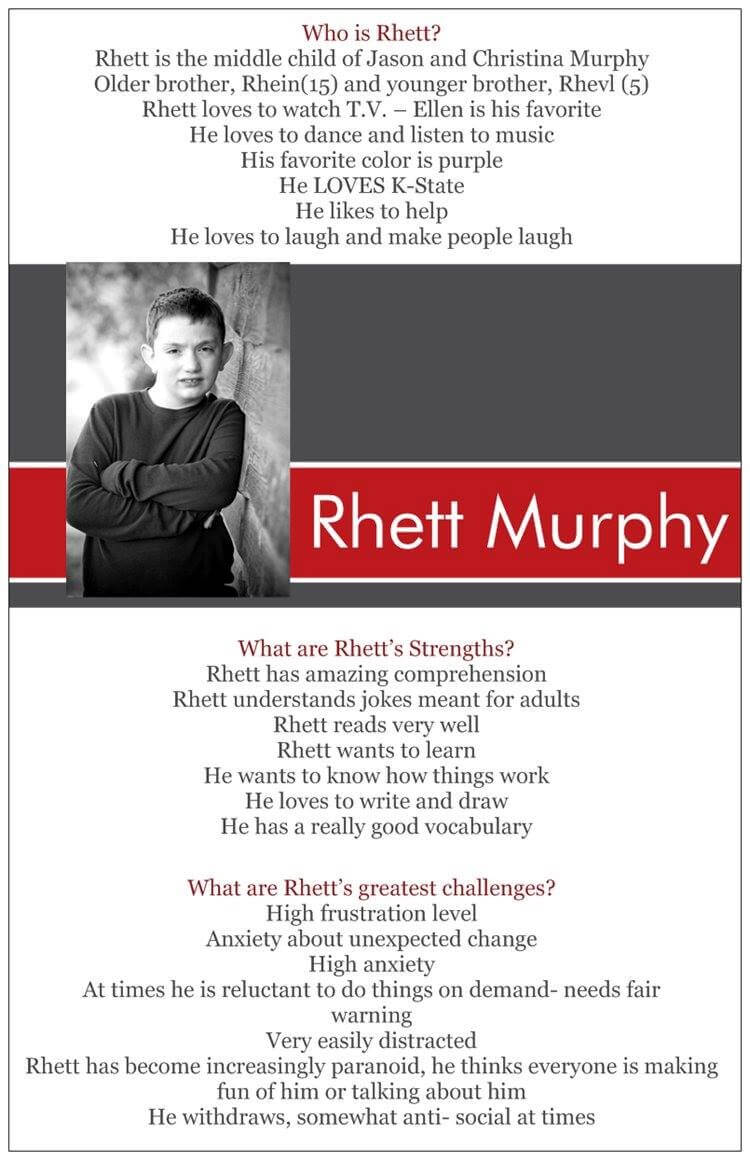
We’d like to thank the Murphy family, Holly Roos, the Welin family and Jayne Dixon Weber for their contributions to this article!
[[1]]This definition was conceptualized by Jean Ayres (1979) an OT and scholar who pioneered what we understand SI to be today.[[1]] [[2]]From Wright’s Law: IDEA does not require parents to “sign” an IEP. Threatening to not sign an IEP does not really mean much. Also, if you do not sign the IEP, others may think you agree to it. You have an absolute right to disagree with the IEP. Do not sit on that right. If you disagree with the IEP, go ahead and sign it, but put a note below or to the side of your name saying that your signature does not mean that you agree with the IEP. – See more at: www.wrightslaw.com/howey/iep.sign.htm[[2]]
Thank you to the National Fragile X Foundation for allowing AXYS to use this content.
Salivary Testosterone in Relation to Social Cognition and Social Anxiety in Children and Adolescents with 47,XXY (Klinefelter Syndrome)
Article Title: Salivary testosterone in relation to social cognition and social anxiety in children and adolescents with 47,XXY (Klinefelter syndrome)
Author: Sophie van Rijn
Date of Publication: July 23, 2018
“Within the 47,XXY group, lower levels of salivary testosterone were significantly associated with higher levels of social anxiety. The correlation was strong, and independent of age and pubertal development. However, salivary levels of testosterone were uncorrelated to social cognitive skills.”
Oxandrolone Treatment Effects on Motor Function, Cognition and Behavior
Article Title: Androgen Treatment Effects on Motor Function, Cognition, and Behavior in Boys with Klinefelter Syndrome
Authors: Judith L. Ross, Nicole Tartaglia, Shanlee Davis, Allan L. Reiss, et al
Date of Publication: June 2017
“This double-blind, randomized trial demonstrates that 24 months of childhood low-dose androgen treatment in boys with Klinefelter syndrome benefited 1 of 5 primary endpoints (visual-motor function). Secondary analyses demonstrated positive effects of androgen on aspects of psychosocial function (anxiety, depression, social problems), without significant effects on cognitive function, or hyperactive or aggressive behaviors.”
Middle School Teacher Spreads X & Y Chromosome Variation Awareness
Brittney Caracciolo writes:
 “I am the Life Skills Support teacher at Phoenixville Area Middle School in Pennsylvania where I teach students with special needs in grades 6-8. My 19-year-old brother has Klinefelter’s Syndrome and I have always gone with my parents to AXYS meetings whenever possible for as long as I can remember. At the last meeting I attended at DuPont Hospital, they mentioned designating the month of May as X & Y Chromosome Variation Awareness Month. The idea occurred to me that, as a teacher, I have a perfect audience to inform people about these chromosome variations. Not to mention, there are probably students in my school that may have a chromosome variation but don’t even know it. I reached out to my superintendent and assistant superintendent about sending information home to families about X & Y Chromosome Variation Awareness month and they thought it sounded very important and recommended that I speak to my building principal. My principal agreed with the idea of spreading awareness and suggested that we turn it into a week-long awareness campaign and involve student council in some of the planning.
“I am the Life Skills Support teacher at Phoenixville Area Middle School in Pennsylvania where I teach students with special needs in grades 6-8. My 19-year-old brother has Klinefelter’s Syndrome and I have always gone with my parents to AXYS meetings whenever possible for as long as I can remember. At the last meeting I attended at DuPont Hospital, they mentioned designating the month of May as X & Y Chromosome Variation Awareness Month. The idea occurred to me that, as a teacher, I have a perfect audience to inform people about these chromosome variations. Not to mention, there are probably students in my school that may have a chromosome variation but don’t even know it. I reached out to my superintendent and assistant superintendent about sending information home to families about X & Y Chromosome Variation Awareness month and they thought it sounded very important and recommended that I speak to my building principal. My principal agreed with the idea of spreading awareness and suggested that we turn it into a week-long awareness campaign and involve student council in some of the planning.

To make it more inclusive of the whole building, we took a week and each day we designated a different disability or set of disabilities to feature. We chose: Apraxia, X & Y Chromosome Variation Awareness, Autism, Down syndrome and mental health awareness. Each day, a student-friendly description of the disability or set of disabilities was read over the announcements, along with a reminder to visit the table set up in the cafeteria for more information. Each day, there was also a specific thing to wear. For instance, Down syndrome day the students wore “crazy” socks and for X & Y Chromosome Variation Awareness, the students wore AXYS stickers that Sandy was kind enough to make us. The response was definitely overwhelmingly positive! 900 students and 50 staff got to learn about these disabilities. Many of them had never heard of X & Y Chromosome Variations before. I had several teachers come to me and tell me that they learned something new. It was also great to see so many students and teachers wearing the AXYS stickers. I even just found one on a student’s water bottle, 2 months after the fact! Additionally, I gave each teacher a set of brochures on each disability/set of disabilities for their own personal information. I think that the impact of ‘Disability Awareness Week’ will be long-lasting and I intend to do this again next year. Overall, I would say that I was very fortunate to have such a successful experience and would love for others to try and do something similar if they can. It was not very difficult and in my opinion it was very effective.
I do have a few tips to help people plan their own awareness campaign:
- Consider your audience. Since I’m in a school with middle-school aged children, it was very important to me to find and make content that would support the students’ understanding. I also sent the AXYS brochures home to the parents but I wanted the students to have an age appropriate idea of the conditions as well.
- Get people to help you. Although I did a lot of the planning on my own, I did get a significant amount of help from student council and the students and para-professionals in my classroom. There is a lot of time-consuming things that go into a campaign once it’s been approved- making posters, setting up a table, organizing people to be at the table, figuring out how to get information out about the campaign, etc. For all of this, you need some type of support or help. However, the really nice thing is that you can make the awareness campaign however big or small that you want it. Your awareness campaign could simply be putting AXYS brochures with information in people’s mailboxes at work or emailing them to colleagues. It does not always have to be extravagant. However, if you get the chance to do something bigger, I think it will stick out to people more.
- My final tip (and this is thanks to Sandy) is to publicize your hard work afterwards. Through publicizing it, you are reaching even more people who might then feel confident that they can help spread awareness too. The more awareness the better and we can all help do our part.”